Learn how to change behavior.
The world's largest collection of resources and data on behavioral science.
Behavior change and behavior design models
MODELS
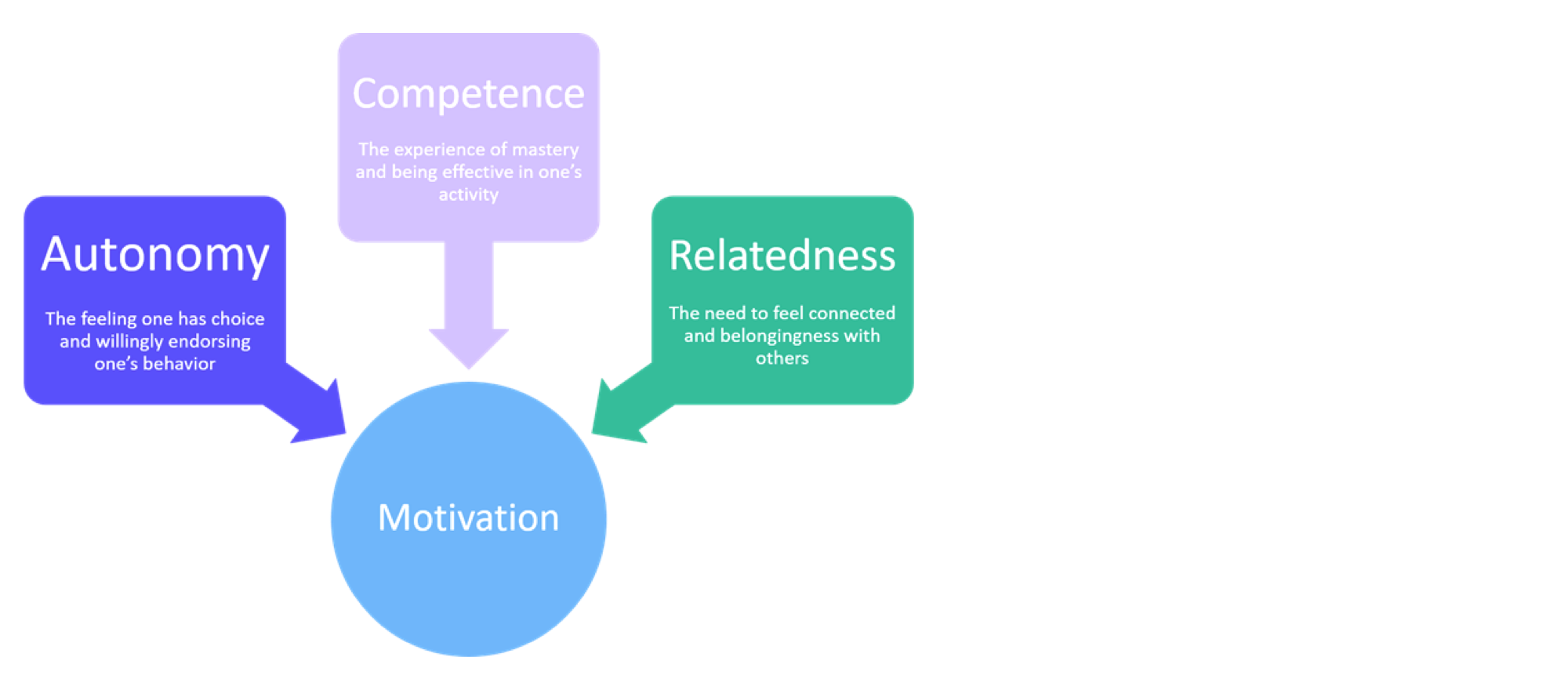
Self-Determination Theory
TYPE
Behavior model
PEOPLE
Richard Ryan, Edward Deci
MODELS
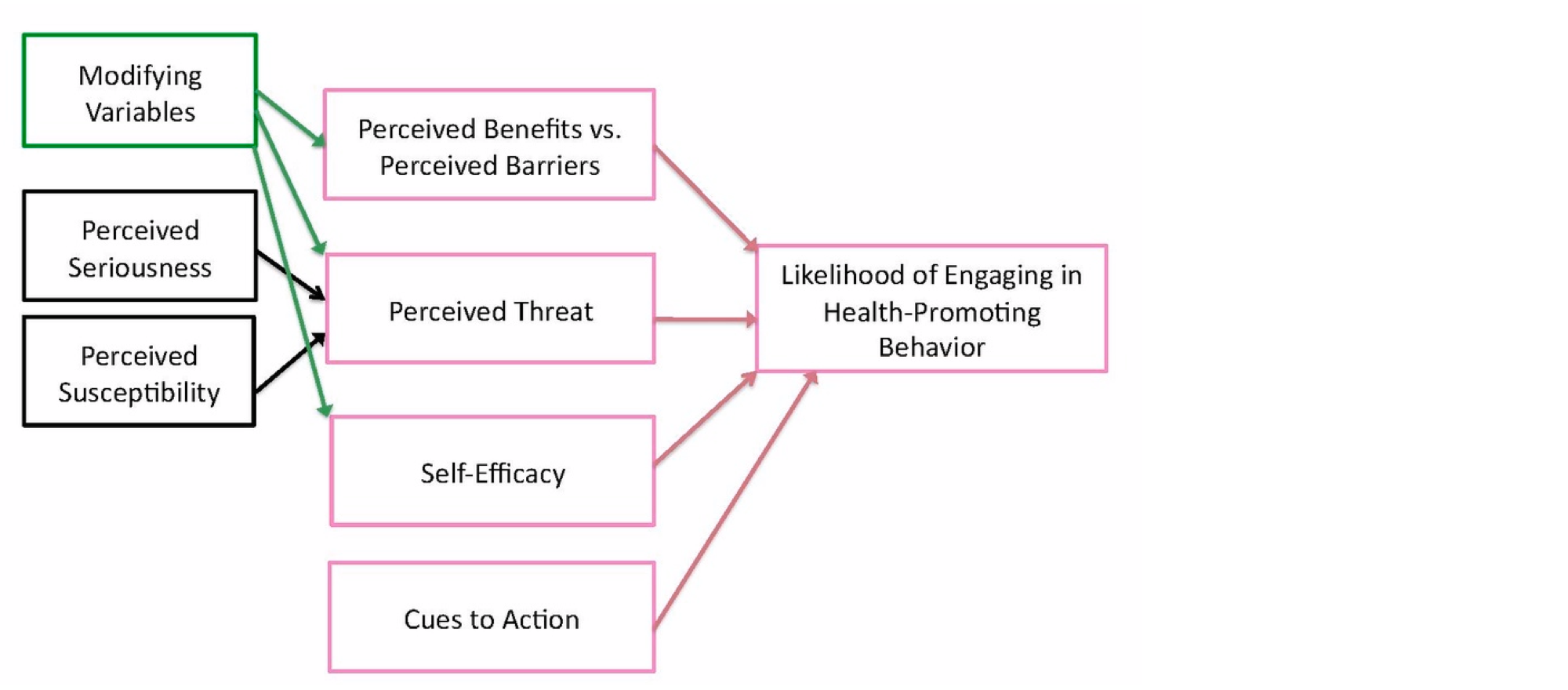
Health Belief Model
TYPE
Behavior model
PEOPLE
Irwin Rosenstock, Godfrey Hochbaum, S. Stephen Kegeles
MODELS
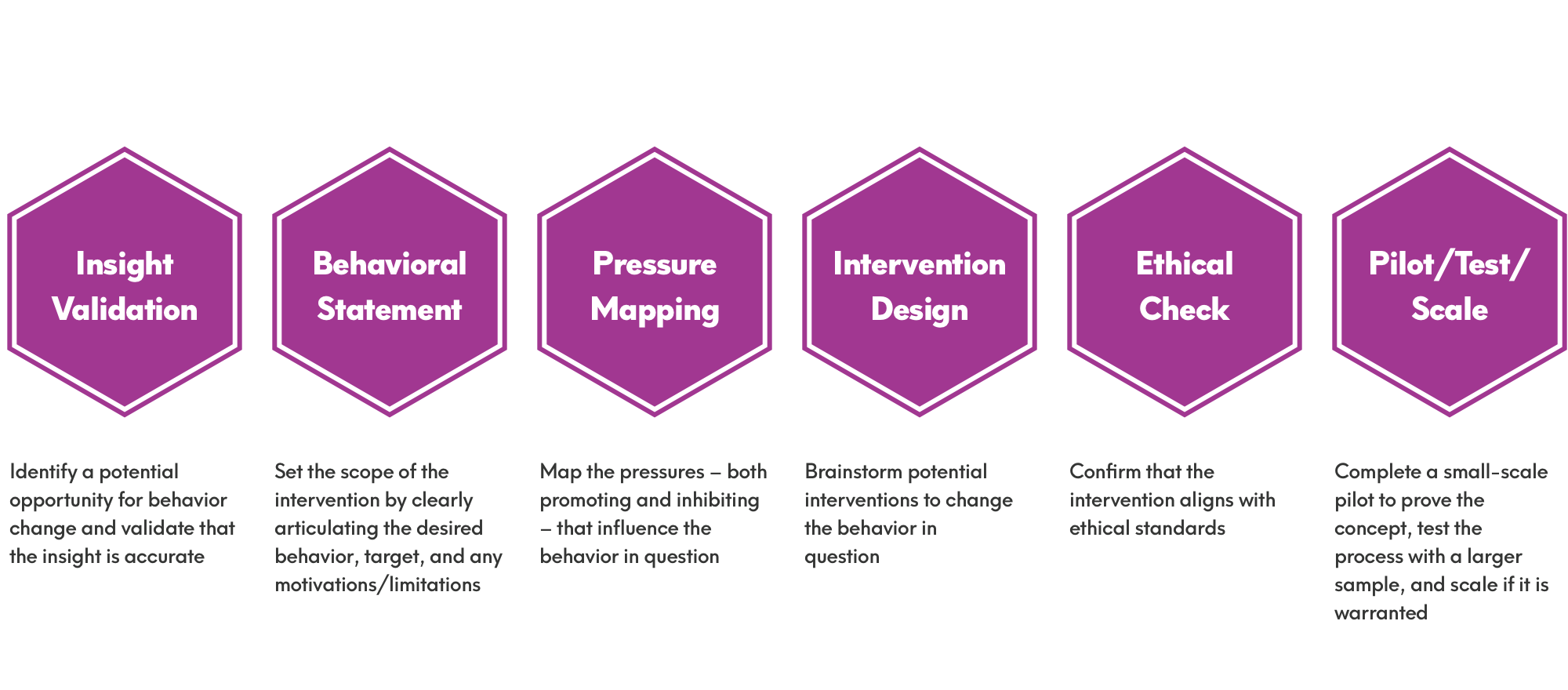
Intervention Design Process
TYPE
Behavior design process / heuristics
PEOPLE
Matt Wallaert
MODELS
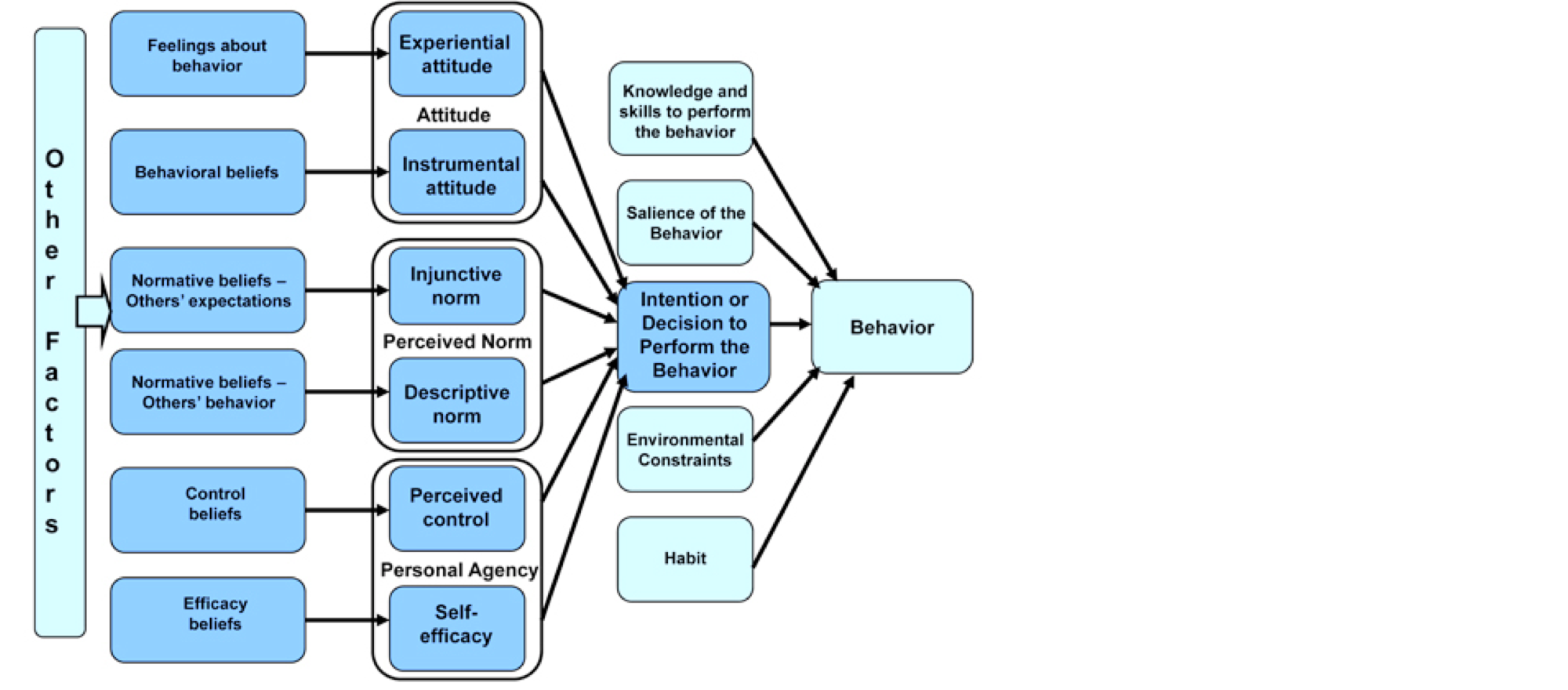
Integrated Behavior Model
TYPE
Behavior model
PEOPLE
Martin Fishbein, Icek Ajzen
MODELS
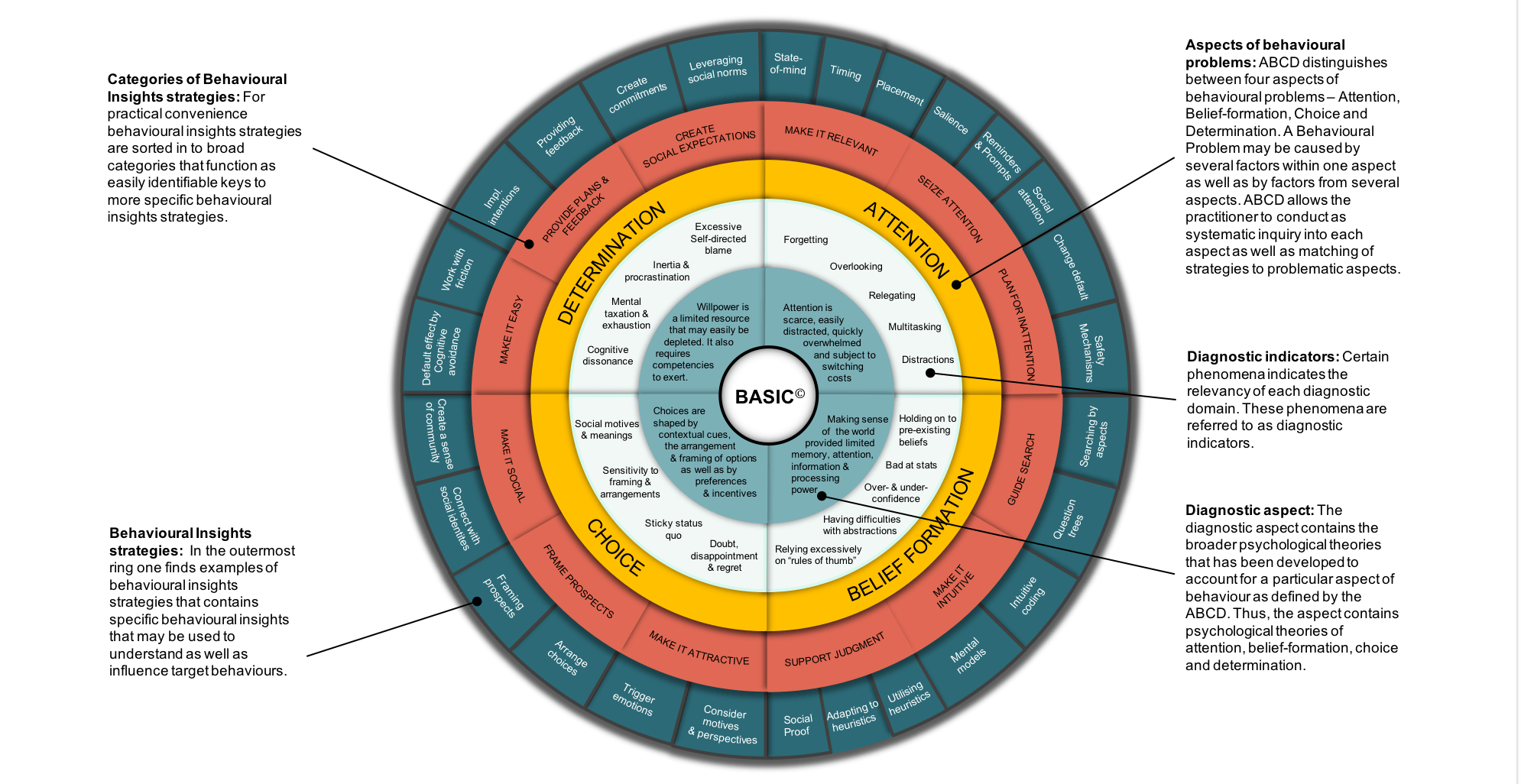
Attention, Belief, Choice, Determination
TYPE
Behavior design process / heuristics
ORGANIZATION
OECD
MODELS
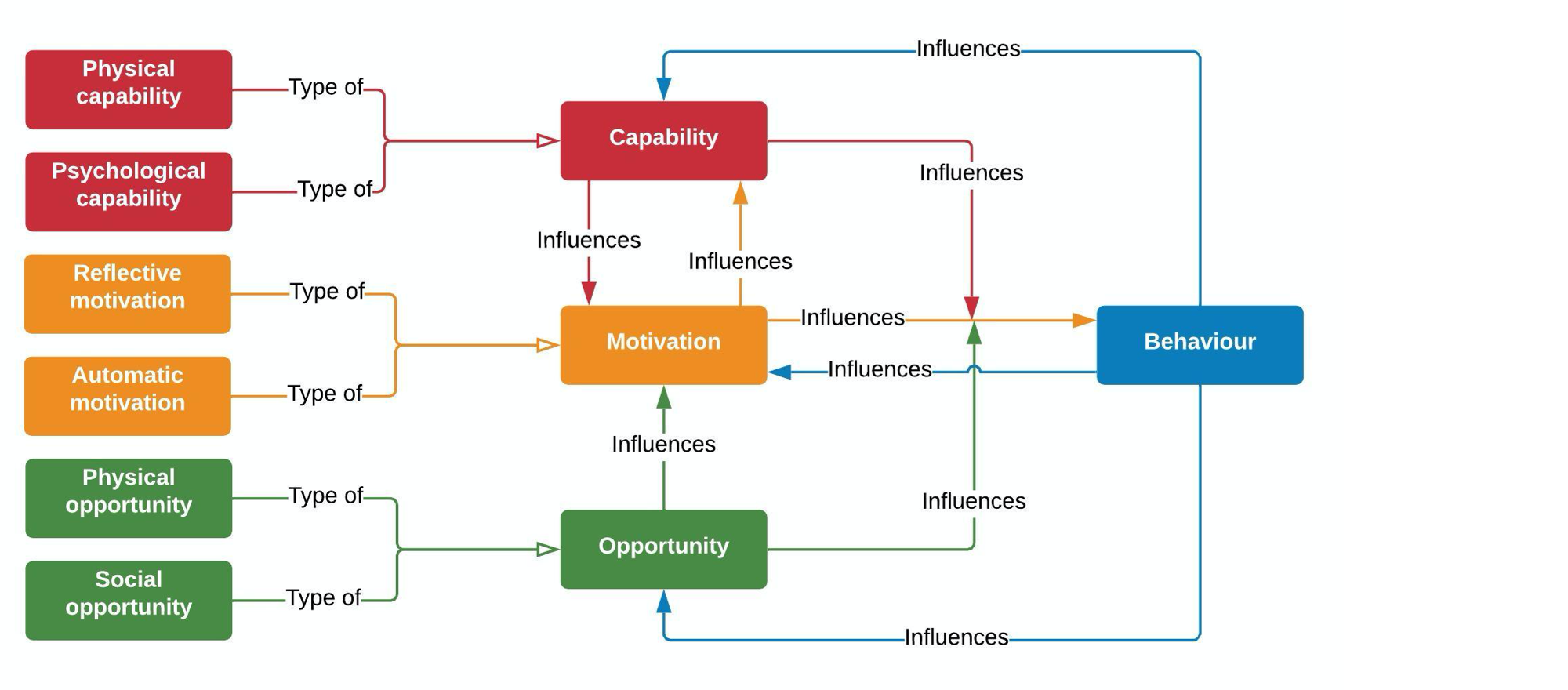
COM-B | Capability, Oppportunity, Motivation → Behavior
TYPE
Behavior model
PEOPLE
Susan Michie, Robert West, Maartje van Stralen
Tactics that change behavior

TACTICS
Checklists
Checklists are an age-old tactic for remembering to do certain tasks. Checklists are sometimes used to measure behaviors that should take place with a certain frequency, e.g. every day or X times per week, and other times, to ensure certain steps are followed every time a person does a complex behavior.For behavior designers, the challenges of checklists often entail choosing the right behaviors, breaking them down to the correct level of granularity for a given population, and serving them up in the proper context or sometimes with personalization. They are likely underutilized and consistently improve the performance of even experts, like pilots and surgeons.

TACTICS
Cognitive Behavioral Therapy (CBT)
Cognitive behavioral therapy (CBT) is a therapuetic approach to improving mental and behavioral health. The core philosophy is that behavior can be modified by noticing and correcting patterns in thought that influence the behavior. Modern CBT is typically associated with Albert Ellis and Alan Beck.The structured and rules-based nature of CBT have made it a popular candidate for digital interventions and application by lightly-trained or even untrained practitioners.

TACTICS
Depression rating
Depression rating simply refers to having someone rate their mood. Often, this may be an informal method like a smiley-face based Lickert scale or choosing a word from a list, rather than using a standardized instrument like the Beck Depression Inventory.

TACTICS
Active Choice
Active choice, sometimes referred to as enhanced active choice or forced choice, refers to removing default options and often increasing the salience of potential decisions through emphasizing the consequences of one or more of the options. Coined by Punam Anand Keller and colleagues in 2011, it was originally intended to address concerns around paternalistic nudging for use in situations where forcing the default option may be considered unethical. In one of the original studies, CVS customers were given the choice to enroll in automatic refills of medications via delivery. The choices they were presented were ""Enroll in refills at home"" vs “I Prefer to Order my Own Refills.”

TACTICS
Automation
Automation refers to having another person, group, or technology system perform part or all of the intended behavior. A prominent example is Thaler & Bernartzi's Save More Tomorrow intervention, which invested a portion of employees' earnings into retirement funds automatically and even increased the contribution level to scale with pay raises. Other examples include automatically scheduling medical appointments so the patient needn't do it themselves and mailing healthy recipe ingredients to the person's home to reduce the burden of shopping.

TACTICS
AI or Chatbot
Using a chatbot or simulated conversational interaction.

TACTICS
Behavioral Activation (BA)
Behavioral activation is a therapeutic approach that typically pairs activity scheduling with either monitoring tools or goal-setting. For example, someone might aim to balance activities they "should" do but underperform, like self-care behaviors, with activities they enjoy. Users of this technique may also track which activities cause certain cognitions or affective states, like those associated with depression.

TACTICS
Commitment Devices
Commitment devices are tools that attempt to bridge the gap between a person's initial motivation to perfrom the behavior and the typical pattern of noncompliance as time goes on.One prominent example is the "Ulysses Pact," where Filipino banking customers were offered the option to enroll in an account where their ability to make withdrawals would be limited. In a study by Ashraf and Karlan (2005), participants with the commitment account saved 81% more than those with typical accounts. There are many other examples of commitment devices. Temptation bundling is a form of commitment device where people only engage in an enjoyable activity when it's simultaneous with an activity they intend to do more (for example, only listening to a certain podcast or audiobook while walking on a treadmill). Pre-paying for a service is a basic form of commitment device, and one used by Dan Ariely when he intended to increase his fruit and vegetable consumption. He paid for a year of biweekly deliveries from a local CSA program up-front.
Products that change behavior

PRODUCTS
AdhereTech
PRODUCTS
ActiveLifestyle

PRODUCTS
Advanced Brain Monitoring

PRODUCTS
10% Happier
Behaviors
Mental Health & Self-Care
Tactics
Reminders, Cues, & Triggers +5 more
PRODUCTS
ALICE
Behaviors
Medication Adherence

PRODUCTS
Aaptiv
PRODUCTS
2Morrow Weight Management Program
Behaviors
Diet & Nutrition, Physical Activity
Tactics
Acceptance and Commitment Therapy (ACT), Behavioral Activation (BA)
Models
Acceptance and Commitment Therapy

PRODUCTS
Acorns
Behaviors
Savings
Tactics
Framing Effects, Reduce Friction or Barriers, Automation +2 more
Research on behavior change
PAPERS
Nutrition education worksite intervention for university staff: application of the health belief model.
BEHAVIOR
Diet & Nutrition
PAPERS
Designing prenatal care messages for low-income Mexican women.
BEHAVIOR
Other
TACTICS
Education or Information
PAPERS
Interrupting pathways to sepsis: Effectiveness of an intervention to reduce delays in timely care for sick children in rural Bangladesh.
BEHAVIOR
Other
PAPERS
Continuous glucose monitoring counseling improves physical activity behaviors of individuals with type 2 diabetes: A randomized clinical trial.
BEHAVIOR
Physical Activity, Disease Management
PAPERS
The effects of a multimodal intervention trial to promote lifestyle factors associated with the prevention of cardiovascular disease in menopausal and postmenopausal Australian women.
BEHAVIOR
Physical Activity
PAPERS
Value-Based Insurance Design Improves Medication Adherence Without An Increase In Total Health Care Spending
PAPERS
The Effectiveness of Prompts to Promote Engagement With Digital Interventions: A Systematic Review.
BEHAVIOR
Other
PAPERS
A comparison of two delivery modalities of a mobile phone based assessment for serious mental illness: native smartphone application vs text-messaging only implementations.
BEHAVIOR
Mental Health & Self-Care
PAPERS
A Digital Diabetes Prevention Program (Transform) for Adults With Prediabetes: Secondary Analysis
PRODUCT
Transform
BEHAVIOR
Physical Activity, Diet & Nutrition